



What good is a treatment if your patient won’t adhere to it?
Some patients may perceive compression therapy or offloading as a MAJOR INCONVENIENCE, as it involves engaging with treatment for a LONG PERIOD OF TIME.1
Low adherence with therapy may results in DELAYED HEALING and poor healing outcomes2.
Healthcare professionnals have an IMPORTANT ROLE to play in explaining :
- The aetiology,
- Why the treatment is important
- Why they should wear compression or offloading continuously
- Etc
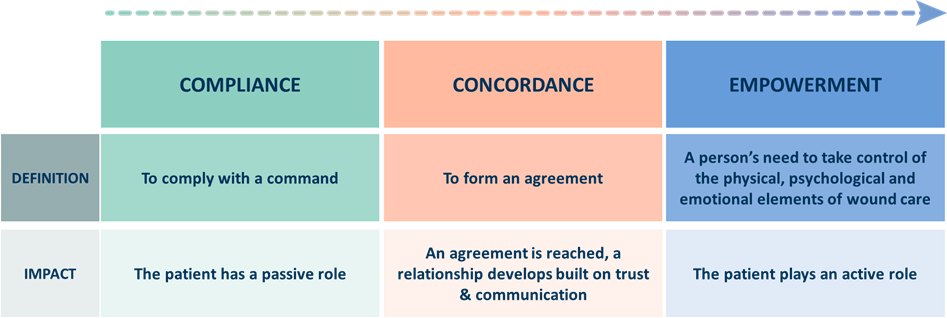
The objective is to enable them to play an ACTIVE ROLE IN THEIR CARE as much as possible.
It’s about moving patients from compliance to CONCORDANCE and, where possible, to promote EMPOWERMENT4
How to improve concordance, and therefore the healing outcome ?
The aim is to treat the person, not just the disease.
The quality of dialogue between the healthcare professional & the patient is key to ensuring that effective treatment is implemented.
The dialogue should also involve the patient’s caregivers, who may play a central role in their care.
