What is Evidence Based Practice ?
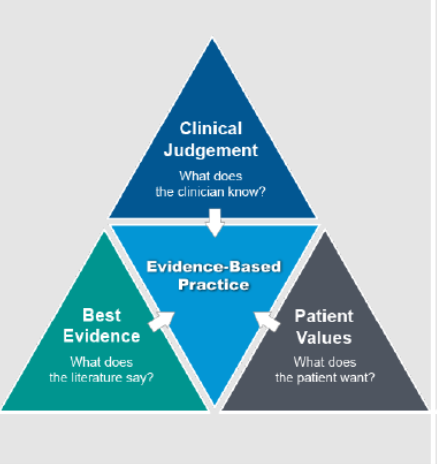
It is the integration of best research evidence with clinical expertise and patient values [Sackett 2001]
– Clinical judgement is acquired through clinical experience and practice.
– Patient values can be assessed through an Inclusive Dialogue with him and/or its caregivers
– Best evidence can be observed from the literature
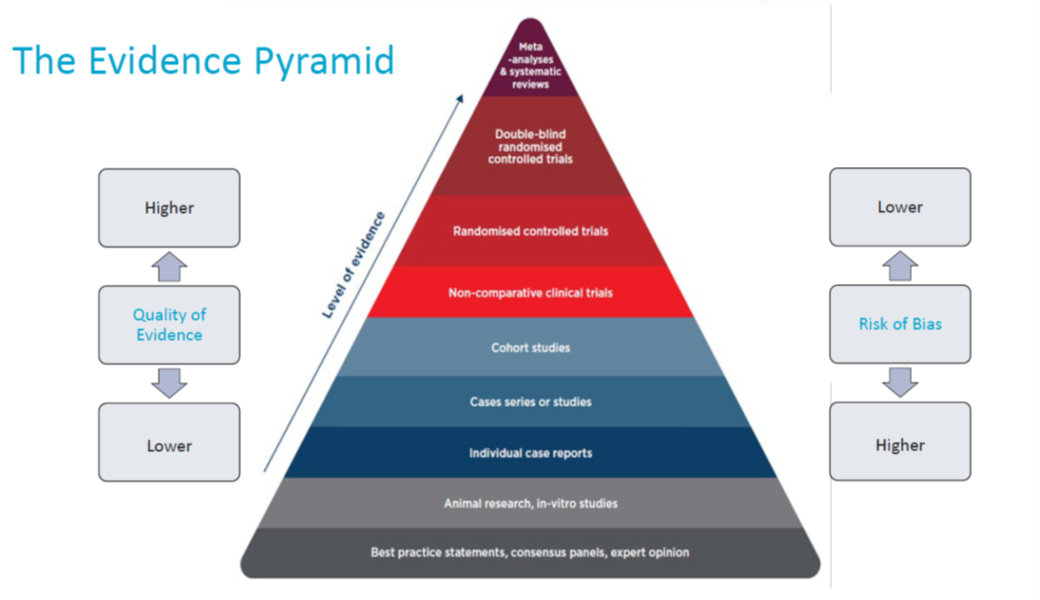
But not all Evidence is equal :
- Some sources of evidence are stronger than others
- Study design play an important role in the quality of the evidence
- Each source of evidence has a specific objective and role to play (ie only RCT – randomised controlled trial can prove the efficacy of treatment)
The critical analysis of the evidence is an essential skill for healthcare professionals. The Evidence Pyramid can help in assessing the quality of the evidence and the risk of bias.
Evidence has therefore a key role in healing patients sooner.
In Urgo Medical we are committed to provide Healthcare Professionals with the best Standard of Care from the beginning so that life can start again for their patients. The standard of care for patients includes a local treatment and an etiological treatment to provide them the best outcomes.
Local care : once the risk of delayed wound healing (comorbidities, risk or local signs of infection) is identified through a Patient-centred Diagnosis, a local treatment can be prescribed :
- If a patient presents with a risk of infection or signs of local infection, a combined antimicrobial and complete cleaning action is required in order to clean the wound from all the elements that support and increase the risk of infection (microbes, exudate, biofilm, slough & other wound debris) – UrgoClean Ag (add link)
- If a patient presents with comorbidities (diabetes, venous insufficiency, advanced age, etc) but no risk or signs of local infection, a specific local treatment from day one is required that will continuously clean, effectively heal and close the wound as soon as possible – avoiding further complications. (UrgoStart Plus – add link)
- With patients with no comorbidities nor risk of infection, the objective is to provide and maintain a moist environment locally while ensuring painfree cares. (UrgoTul range – add link)
Etiological treatment : in patients presenting with with diabetes, venous insufficiency or limited mobility, an etiological treatment is necessary to ensure healing.
For patients with a venous leg ulcer: the recognized STANDARD OF CARE is compression therapy.1-3
Yet there are many challenges to overcome to select the best compression treatment: